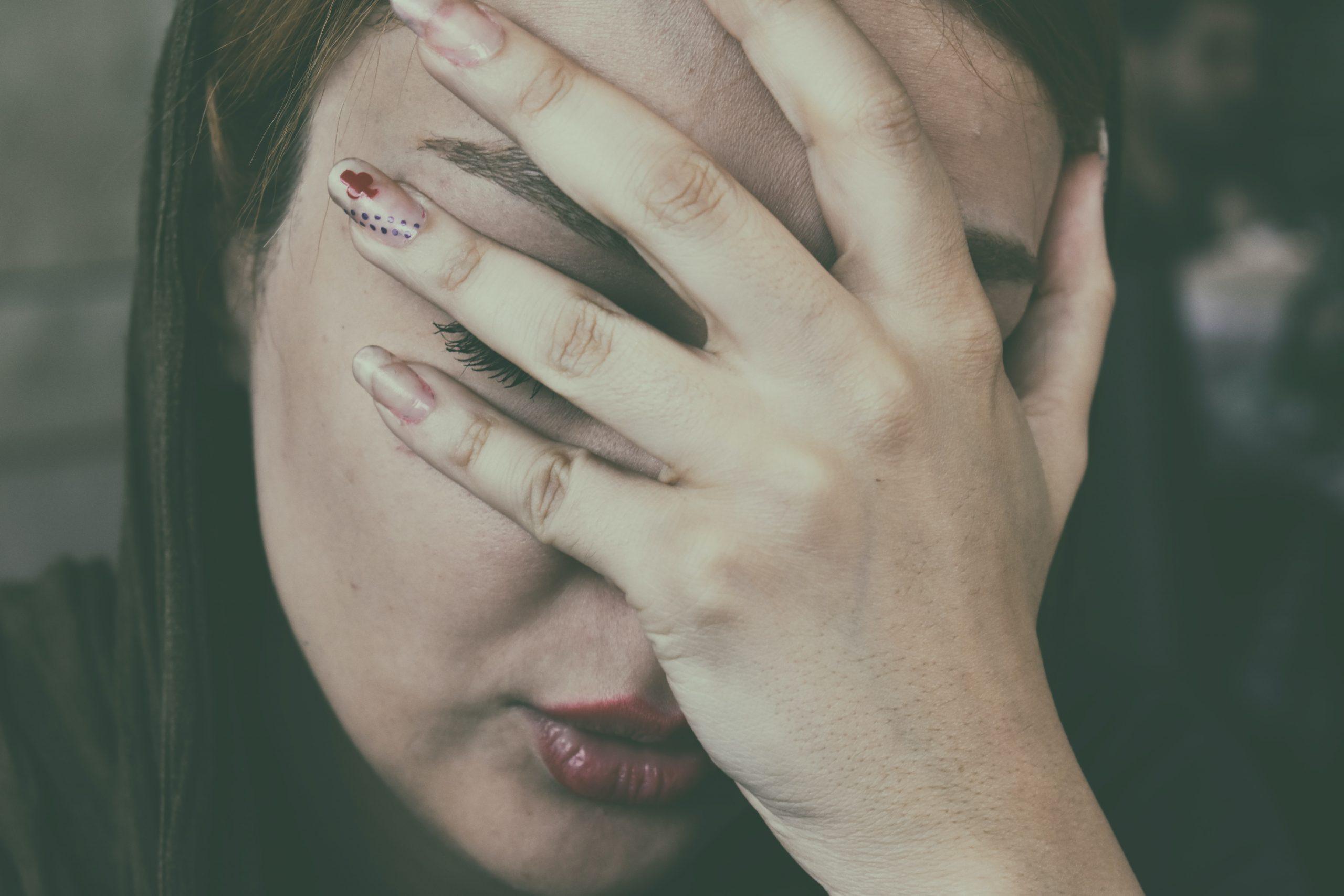

Gender differences in the experience of pain have been widely reported, with females generally reporting more frequent clinical pain and demonstrating greater pain sensitivity. Biological, psychological, and sociocultural factors act interdependently to influence pain response.
Stereotypical pain

Both males and females endorse gender stereotypical views on pain, which affect their pain responses. Previous research indicates that men typically tolerate more pain in experimental settings than women. For example, both males and females believed that a typical man should tolerate more pain than a typical woman.
Masculinity is considered as having high pain threshold and pain tolerance.
But, many painful conditions are more prevalent in women than men including temporomandibular disorders, migraine, tension‐type headache, fibromyalgia, and irritable bowel syndrome. Gender stereotypes specific to pain do not reflect masculinity and femininity in a broader sense.
What’s commonly known?
- Women have greater sensitivity to pain.
- Gender role appears to influence response to pain.
Tolerance changes in front of opposite sexes.
In a previous study, male patients reported higher pain scores to male practitioners when experiencing relatively low pain levels, and both male and female patients reported higher pain scores to female practitioners when experiencing relatively high pain levels.

In another study, it was found that the lower pain report in male to female clinicians was not mediated by changes in autonomic parameters, but may be due to psychosocial factors. One more study concluded that males reported significantly less pain in front of female clinicians than male clinicians. The difference in female subjects was not significant although they tended to report higher pain to the male clinicians.
Opposite gender doctor may increase the tolerance level.
Pieces of evidence have been seen that a significant interaction of clinician gender and patient gender on pain tolerance indicated that patients also tolerated pain longer when they were tested by a clinician of the opposite sex.
In a recent study, it was found that females appeared to under-report their pain responses in front of males clinicians. It was also concluded
- that females reported lower sharpness ratings to male than female (clinicians)
- females exaggerated pain, but not males; and
- in females, lower pressure-pain thresholds were associated with higher pain exaggeration in front of males.
Young females no longer perceive themselves as the ‘weaker sex’ but equal to males who are of similar age and status.
These findings indicate that the clinicians’ gender and the patients’ pain exaggeration influence pain tolerance, particularly in females. So women visiting male clinicians may report lower pain.