
Imagine if you have clitoris arousal which is persistent for days. And uncontrolled orgasm or on a verge of orgasm for hours. Wouldn’t it be great? Wouldn’t you enjoy such arousal?
The answer is NO!!! Persistent clitoris arousal will lead to swelling and pain in the clitoris area. Because the arousal has nothing to do with your interest in having sex nor your libido to have sex with someone. It is unwanted and prolonged arousal that leads to pain and discomfort. It affects all ages of women, studies have shown women of age 26 to 47 suffering from such disorders.

2019 ISSWSH consensus expert opinion on criteria and characteristics of persistent genital arousal disorder/genito-pelvic dysesthesia (PGAD/GPD)
| Criteria | persistent or recurrent, unwanted or intrusive, distressing sensations of genital arousal |
| duration of ≥3 months | |
| may include other types of genito-pelvic dysesthesia (eg, buzzing, tingling, burning, twitching, itch, pain) | |
| most commonly experienced in the clitoris but also in other genito-pelvic regions (eg, mons pubis, vulva, vestibule, vagina, urethra, perineal region, bladder, and/or rectum) | |
| may include being on the verge of orgasm, experiencing uncontrollable orgasms, and/or having an excessive number of orgasms | |
| not associated with concomitant sexual interest, thoughts, or fantasies | |
| Associations | limited resolution, no resolution, or aggravation of symptoms by sexual activity |
| compromised orgasm quality (eg, aversive, impaired, altered frequency, intensity, timing, and/or pleasure) | |
| aggravation of genito-pelvic dysesthesia by certain circumstances (eg, sitting, car driving, music or sounds, general anxiety, stress, or nervousness) | |
| despair, emotional lability, catastrophization, and/or suicidality | |
| on physical examination, absent evidence of genital arousal (genital lubrication, swelling of clitoris or labia) |
Persistent clitoris arousal with unbidden and unwelcomed orgasms.
Persistent genital arousal disorder (PGAD) is unwanted genital arousal that occurs in absence of sexual interest and desire.
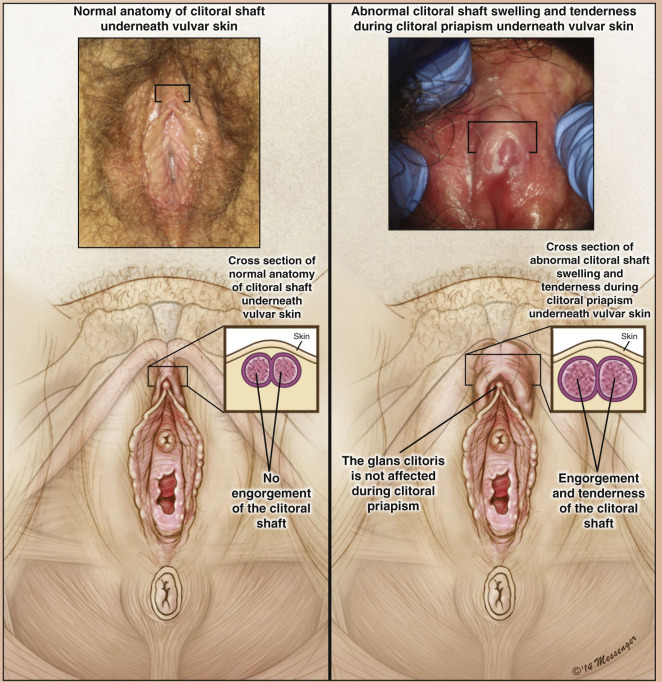
Priapus, the Greek god of plenty, represented the reproductive power of the male. But priapism, a painful permanent erection, has little to do with procreation. Nor is it restricted to men or women.
Normal erections are produced by a sudden influx of blood to the penis/ clitoris, which becomes stiff. The influx occurs when certain muscles relax, allowing blood to enter via the arteries, while veins are pinched tight, blocking the blood’s exit. Problems with either exit or entry of the blood can cause priapism.
A subtle and intermittent clitoral priapism may favor the feeling of arousal persistence and elicit unbidden and unwelcomed orgasms.
Drug-induced unusual erectile activity in the clitoris.
Clitoral priapism can be secondary to hematological disorders, neurologic disorders, or adverse reactions from medications such as antipsychotics, antidepressants, antihypertensives, or recreational drugs.
There are cases where it has been reported that the use of certain drugs, resulted in persistent clitoris arousal for more than 24 hours. A case of painful priapism of the clitoris lasting 24 hours, which was believed to be pathophysiologically associated with the administration of trazodone hydrochloride, a heterocyclic antidepressant. A case report of a 47-year-old woman presented complaining of vulvar and clitoral pain, discovered to be attributed to the use of trazodone hydrochloride,
Besides the trazodone, another therapy like nefazodone, bupropion, citalopram, and olanzapine use have shown doubts of causing clitoral priapism.
Recommended treatments.
Priapism of the clitoris is a condition that may develop during therapy with certain medications, specifically those possessing a strong alpha-adrenergic blockade. Conditions altering blood flow to the clitoris may also predispose to developing this condition.
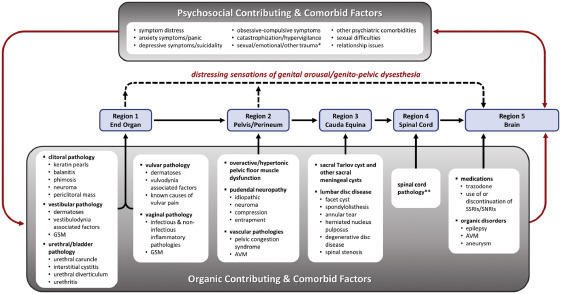
Factors are categorized as originating from 5 separate regions that may be successively modified through afferent nerve pathways.
Off-label pharmacological treatment strategies for symptom control of PGAD/GPD
| Category | Commonly Prescribed medications | Potential Dosing Regimen | ||
|---|---|---|---|---|
| Anticonvulsants and non-opioid inhibitors of neurotransmission | carbamazepine gabapentin pregabalin topiramate lamotrigine oxcarbazepine |
100 mg po, bid 100 mg po, tid; (maximum dose of 3,600 mg/d) 50 mg po, tid (maximum dose of 300 mg/d) 100 mg po, bid 50 mg po, qd; increase as needed 300 mg po, bid |
||
| Benzodiazepine GABA-ergic activators | clonazepam | 0.25 mg bid | ||
| Non-benzodiazepine GABA-ergic activators | zolpidem | 1 mg (compounded) tid or qid | ||
| Opioid Inhibitors of neurotransmission | tramadol hydrocodone |
50 mg po, bid or tid 5–10 mg po, qd (in combination with acetaminophen, 325 mg) |
||
| Tricyclic antidepressants | amitryptiline clomipramine desipramine nortriptyline |
10 mg po qd (maximum dose of 150 mg/d) 25 mg po, qd (maximum dose of 250 mg/d) 100 mg po, qd (maximum dose of 300 mg/d) 25 mg po, tid (maximum dose of 150 mg/d) |
||
| SSRI/SNRI | duloxetine paroxetine |
20 mg po, bid (maximum dose of 60 mg/d) 12.5 mg po, qd (maximum dose of 50 mg/d) |
||
| Dopamine antagonists or lowering agents | paliperidone risperidone varenicline |
6 mg po, qd (maximum dose of 12 mg/d) 2 mg po, qd (maximum dose of 16 mg/d) 0.5 mg po, qd (maximum dose of 2 mg/d) |
||
| Specific Indications | ||||
| Hyperthyroidism | methimazole propranolol |
5 mg po, tid 40 mg po, bid (starting dose) |
||
| Restless leg syndrome | ||||
| Dopamine agonist | pramipexole | 0.125 mg po, tid | ||
| Pelvic floor dysfunction | ||||
| Benzodiazepine | diazepam | 2.5–10 mg, qd, vaginal/rectal suppository; in conjunction with physical therapy | ||
| GABA agonist | baclofen | 20 mg, qd, vaginal/rectal suppository; in conjunction with physical therapy | ||
| Anti-cholinergic (neurotoxin) | botulinum toxin A | 50–200 units, im, every 3 months | ||
| Menopause | ||||
| Sex steroid hormone receptor agonists | systemic estradiol systemic testosterone systemic progesterone systemic estradiol & progesterone local vestibular/vaginal |
biologically identical estradiol biologically identical testosterone at one-tenth approved dose for men biologically identical progesterone biologically identical estradiol and progesterone compounded estradiol (0.01–0.03%)/testosterone (0.1%), topical to vestibule, qd local estradiol local DHEA suppository |
||
Consult your doctor before starting any medication